
Clascoterone, the topical androgen receptor antagonist being developed for hair loss under the name Breezula by Cassiopea, has become one of the most discussed drugs in the hair loss field over the past two years. The enthusiasm is understandable. A compound that blocks DHT's effects directly at the follicle level, applied topically, without the systemic exposure that makes finasteride and dutasteride risky for some patients, sounds almost too good to be true. After reviewing the Phase 3 data, I'd argue the reality is somewhere between the hype and the sceptics.
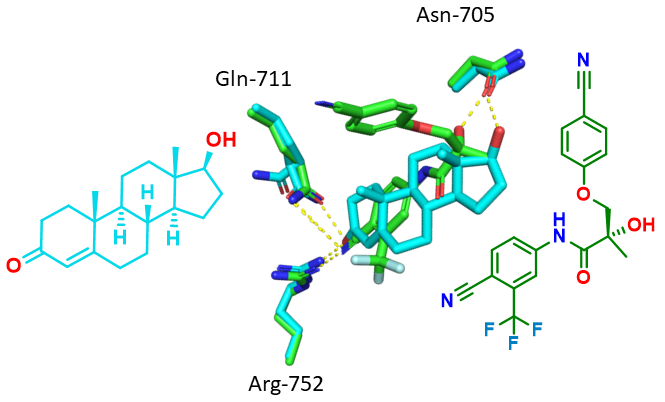
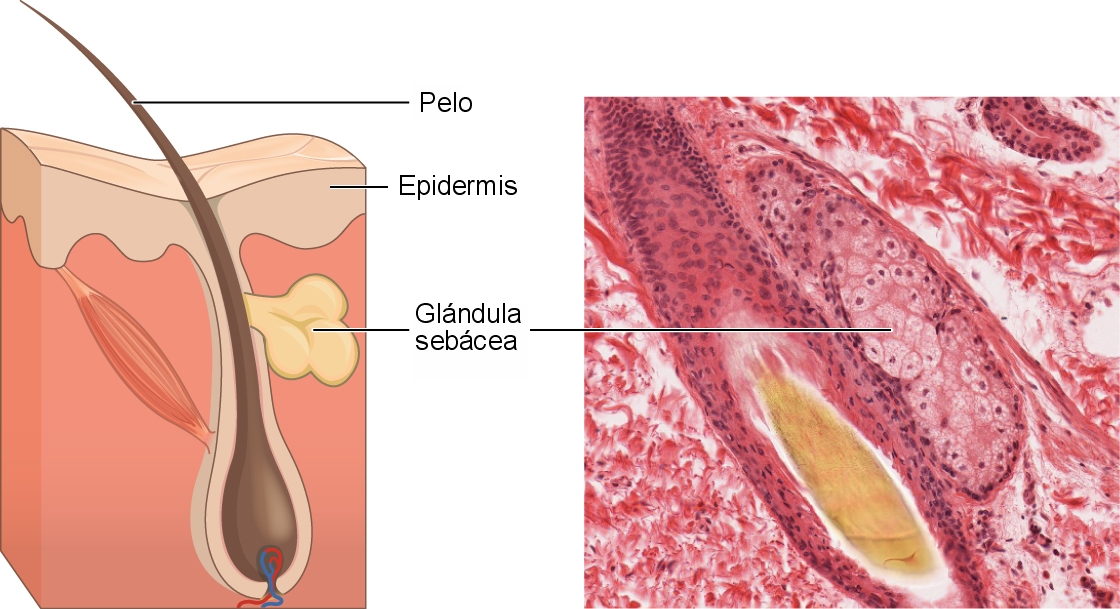
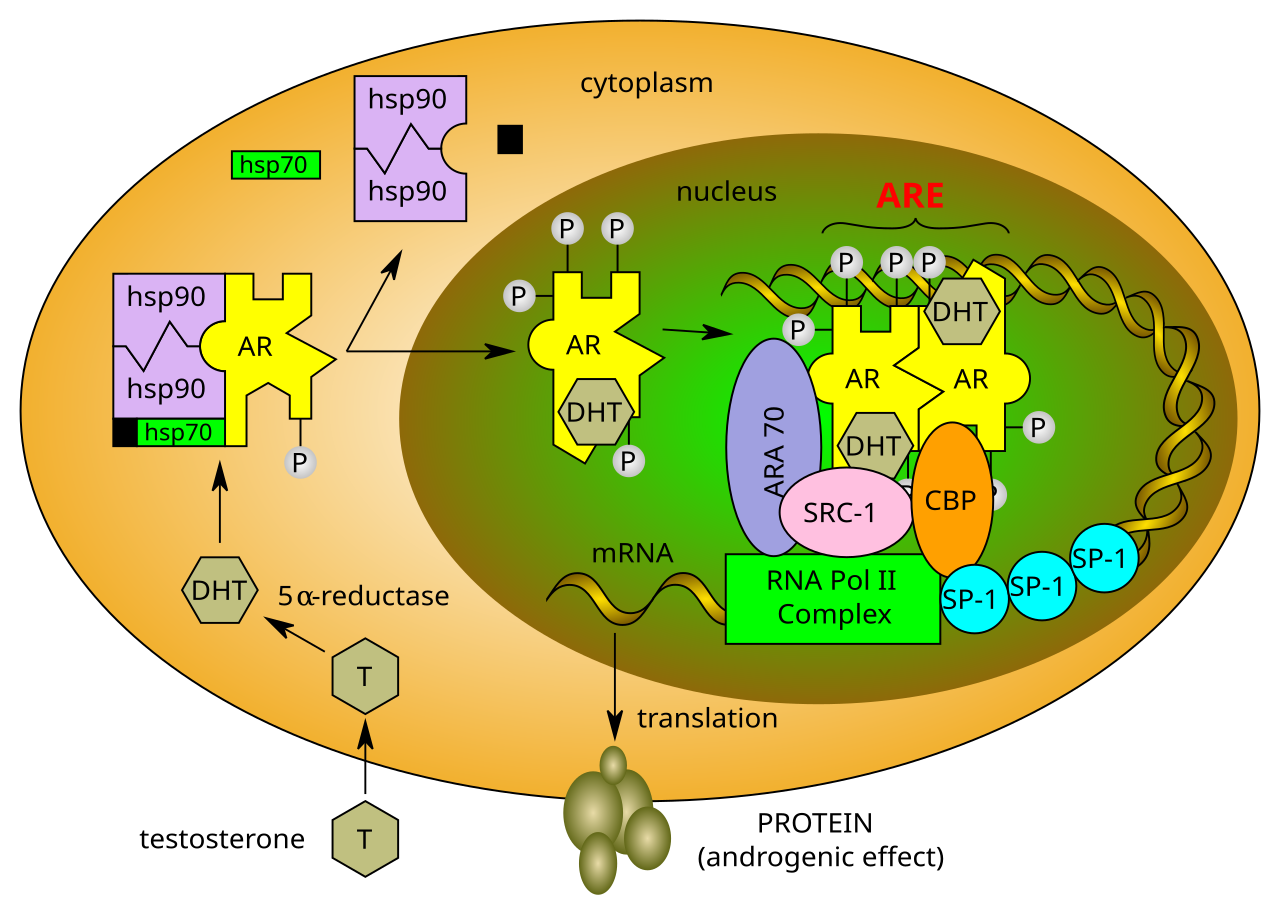
The mechanism is well-established. Clascoterone competitively antagonises the androgen receptor, the same receptor that DHT binds to and uses to miniaturise follicles in genetically susceptible scalp zones. The drug is already FDA-approved as Winlevi cream for acne, where it works by the same mechanism on sebaceous glands. The acne indication gave researchers useful safety data and confirmed that topical clascoterone doesn't measurably suppress serum testosterone or DHT in men, which is the key advantage over oral antiandrogens.
The Phase 3 BREEZULA trial enrolled over 900 men with androgenetic alopecia across multiple sites in Europe and the US. After 12 months of twice-daily application of 7.5% clascoterone solution, the treated group showed a statistically significant improvement in target area hair count compared to placebo, approximately 8.4 additional hairs per cm² in the clascoterone arm versus 2.1 in the placebo arm. Hair width measurements and global photography assessments supported the primary endpoint.
Here's where the nuance matters. An 8.4 hair/cm² improvement is real. Statistically and histologically, it's real. But in clinical practice, it's modest. For context, minoxidil 5% in Phase 3 trials typically produced 15–20 additional hairs per cm² in comparable measurements. Finasteride produced 17–23. Clascoterone's effect size is roughly half that of established treatments, which isn't nothing, but it's not the breakthrough that some commentators have described.
The patient-reported outcomes were mixed. In the investigator's global assessment, 22% of clascoterone patients showed a rating of "improved" or "greatly improved" compared to 11% on placebo, statistically significant but relatively modest in absolute terms. Patient-reported assessments of satisfaction tracked similarly.
The safety profile is genuinely clean. No meaningful systemic androgen suppression, no reports of sexual dysfunction, no elevated liver enzymes. The main adverse events were mild skin reactions at the application site, dryness and irritation in roughly 8% of participants. That tolerability data matters enormously for younger men who are reluctant to start systemic treatment.
My assessment: clascoterone will likely receive FDA approval for androgenetic alopecia within 18 months if Cassiopea files the NDA. It will occupy a useful niche as a non-systemic option for men who can't or won't take finasteride. The more interesting question is whether it becomes a platform for combination therapy, clascoterone plus minoxidil, or clascoterone plus a Wnt activator, where the synergy between mechanisms could produce effects larger than either drug alone. That trial has not yet been run.


Discussion (2)
Rachel K.
2 months ago
Finally some honest analysis on this. The marketing around Breezula has been way ahead of what the data actually shows.
James_NW3
2 months ago
I'd try this immediately if it comes to market. The finasteride side effect profile scared me off at 28 and I've been on minoxidil alone since.
Join the discussion
Free account. Read, like, save, and comment on every article.