
Ritlecitinib got FDA approved for severe alopecia areata in June 2023, and most of the press coverage stopped at "another autoimmune drug." Fine, that's accurate. But it misses what was actually interesting about it. The drug is sold as Litfulo, and if you spend any time with the ALLEGRO Phase 2b/3 data, you start to understand why hair loss researchers wouldn't shut up about it for the rest of that year.

Ritlecitinib inhibits JAK3 and TEC kinases. The headline number from ALLEGRO: 31% of patients on the 50mg dose hit a SALT score of 20 or less. That means 80% or more scalp coverage. Placebo got 2%. A gap that wide is genuinely unusual in autoimmune disease, and it would matter on its own. What makes it bigger is that the mechanism isn't specific to alopecia areata.
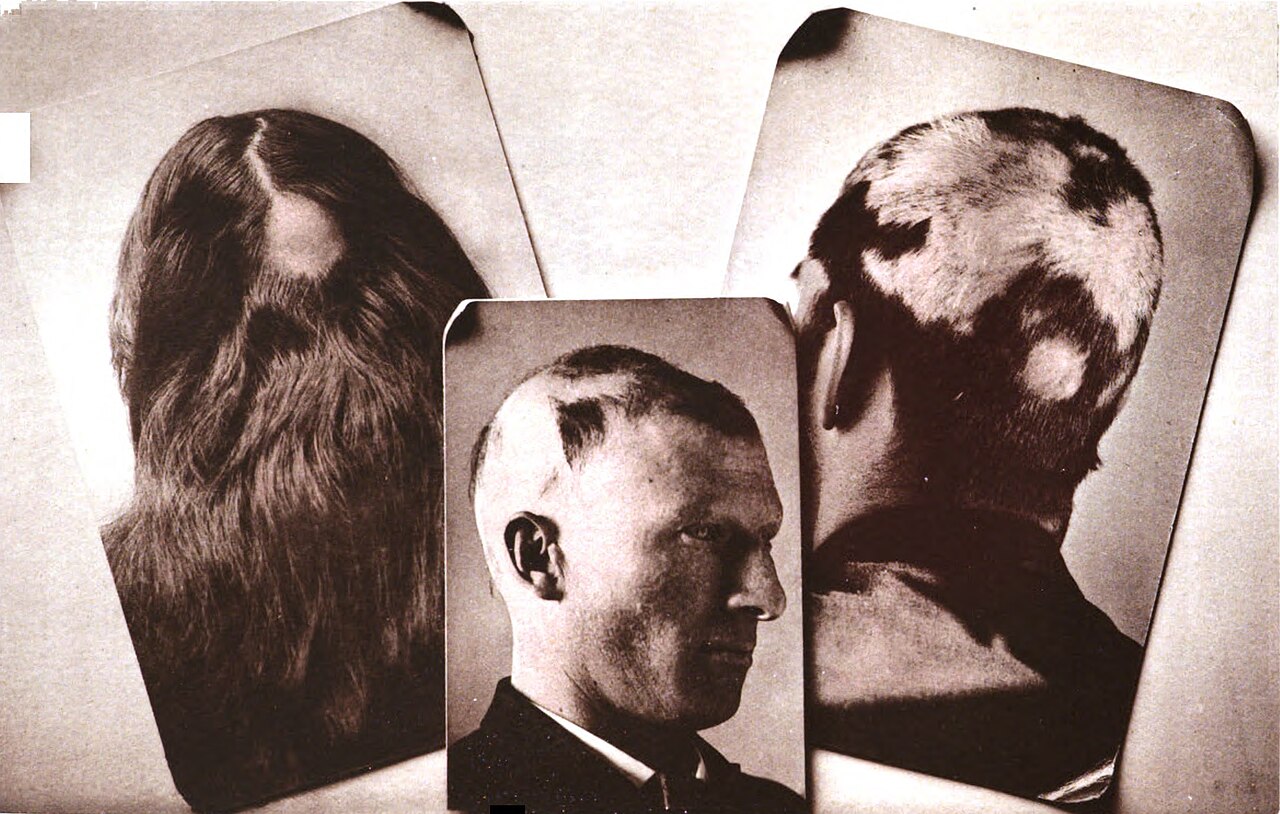
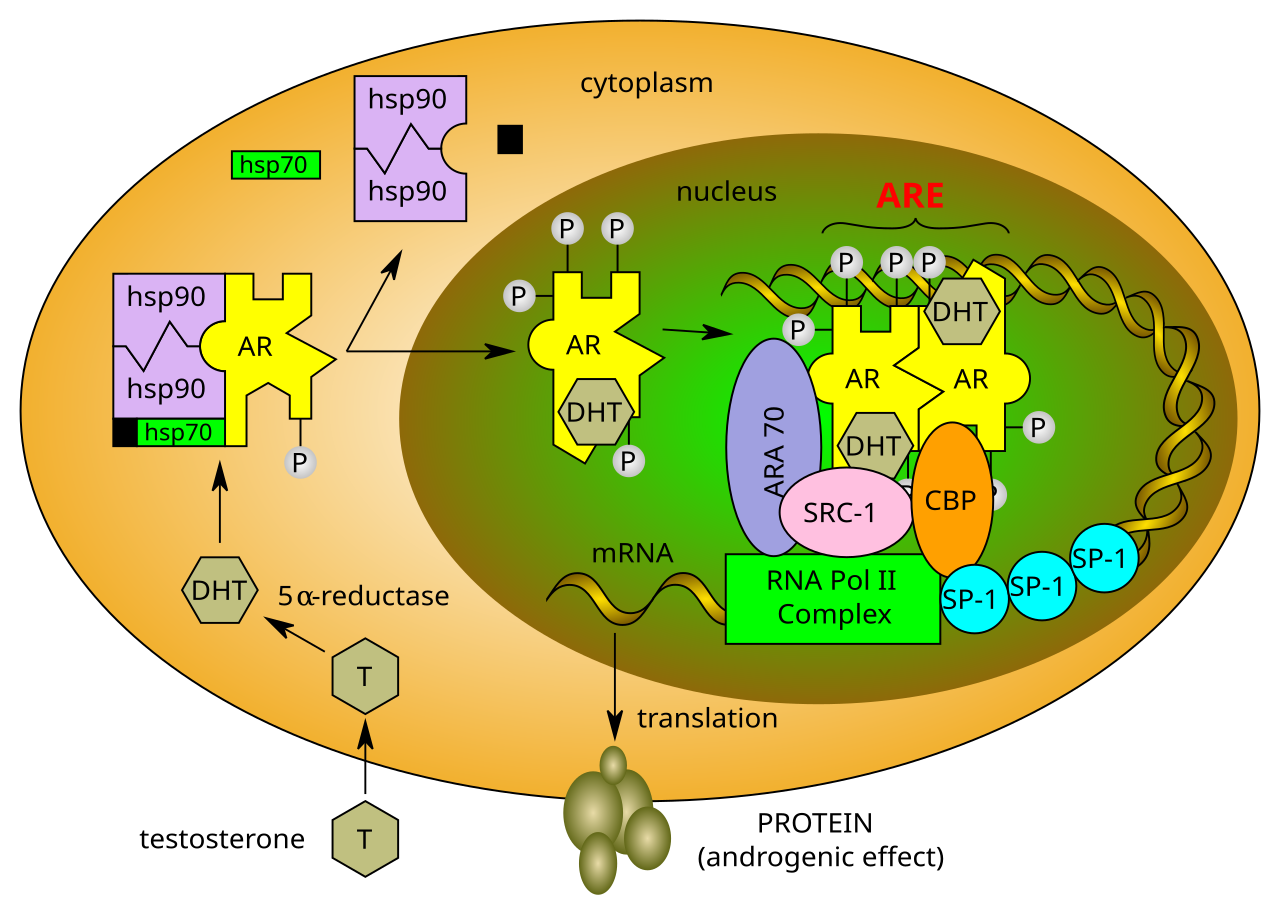
JAK inhibitors block the Janus kinase pathway, which is what drives the immune attack on follicles in alopecia areata. For decades the assumption was that pattern baldness, androgenetic alopecia, was a totally separate thing. Hormonal, genetic, nothing to do with the immune system. That picture has been falling apart for the last few years.
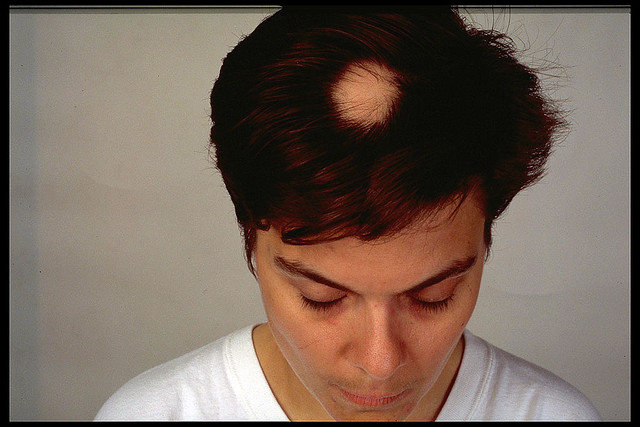
Work published in Nature Immunology in 2022 by Christos Zouboulis and colleagues at Brandenburg Medical School documented meaningful immune infiltration around follicles in androgenetic alopecia scalps, T-cell activity that mirrors, in a milder form, what's seen in alopecia areata. The implications are uncomfortable for the field because they suggest pattern baldness has an inflammatory component that nobody has been adequately treating.

This is where ritlecitinib gets interesting beyond its approved indication. Pfizer is not sitting still. Investigator-initiated studies looking at JAK inhibition in androgenetic alopecia have been quietly accumulating. A small 2024 open-label study out of Seoul National University Hospital found that low-dose ritlecitinib produced measurable follicle density improvements in androgenetic alopecia patients who had failed minoxidil, not dramatic results, but statistically significant in a cohort where nothing was expected to move.
The challenge, as always, is safety. JAK inhibitors carry a class warning for serious infections, malignancy risk, and cardiovascular events, a warning added after the baricitinib arthritis data. For a cosmetic condition, that risk-benefit calculation is genuinely difficult. Ritlecitinib's kinase selectivity profile is actually narrower than older JAK inhibitors like tofacitinib, which theoretically reduces systemic exposure. The 50mg dose used in alopecia areata trials showed a cleaner safety signal than predecessors, though the long-term data beyond two years remains thin.
What the ritlecitinib approval really did was validate the entire JAK pathway as a credible target in hair biology. That validation has attracted serious research funding. Eli Lilly's lebrikizumab, an IL-13 inhibitor, is now being explored in hair loss contexts. Concert Pharmaceuticals developed CTP-543, a deuterated form of ruxolitinib specifically designed for scalp application, reducing systemic absorption. The topical route matters enormously: if you can get a JAK inhibitor to act locally on the follicle without significant systemic exposure, the safety calculus changes completely.
I've been tracking the CTP-543 data closely. The Phase 3 THRIVE-AA1 and THRIVE-AA2 trials showed 41.5% and 34.5% of patients achieving SALT ≤ 20, respectively. Those are respectable numbers. Importantly, the topical delivery kept plasma concentrations well below levels associated with systemic JAK inhibitor side effects.
The 2030 picture is becoming clearer: combination protocols that pair a topical JAK inhibitor with either minoxidil or a Wnt pathway activator could address both the inflammatory and the androgenic components of hair loss simultaneously. No single study has tested this yet. But the biology supports it, and the drug pieces are now available. The question is whether anyone will run the trial.


Discussion (3)
Marcus T.
2 months ago
Been on ritlecitinib for 4 months for AA and the regrowth is real. Curious whether the androgenetic data will eventually get it a second approval.
Priya S.
2 months ago
The immune infiltration finding in androgenetic alopecia is the part that keeps getting overlooked. If pattern baldness has an inflammatory component, that changes the entire treatment model.
DrewFromAustin
2 months ago
Has anyone looked at whether the topical version stacks with low-dose oral minoxidil? Feels like that's the obvious next experiment.
Join the discussion
Free account. Read, like, save, and comment on every article.